
Myopia Epidemic
A closer look at pediatric myopia
Myopia is a chronic, progressive disease growing in both prevalence and severity.1

Myopia is expected to affect more than 50% of the world’s population by 20501

Myopia can interfere with children’s quality of life2,3

Myopia can lead to severe ocular health problems later in life4
The prevalence of myopia in North America has increased 50%, from 28% to 42% over the last two decades.1 Among Canadian school children aged 11-13, almost 30% have myopia.5 Two-thirds of Eye Care Practitioners (ECPs) say the presence of myopia among children in their practice has increased over the past 5-10 years†, and 81% of ECPs agree that myopia is one of the biggest problems impacting children’s eyesight today.§
Standard of Care
The World Council of Optometry and Canadian Association of Optometrist have passed a resolution that declares support for myopia management as standard of care.6
Evidence-based standard of care combines three main components:
![]()
Mitigation
Optometrists educating and counselling parents and children, during early and regular eye examinations, on lifestyle/dietary/other factors to prevent/ delay onset of myopia
![]()
Measurement
Optometrists evaluating the status of a patient during regular comprehensive vision and eye health examinations
![]()
Management
Optometrists addressing patients’ needs of today by correcting myopia, while also providing evidence-based interventions that slow the progression of myopia, for improved quality of life and better eye health today and into the future

What's causing the rising prevalence of myopia?
The upward incidence of myopia in today’s children can be attributed to different factors, and is occasionally the result of a combination of these factors:
Genetics
Family eyesight history plays a role in a child’s risk of myopia. The likelihood of children developing myopia is:
![]()
1 in 2
when both parents are myopic10
![]()
1 in 3
when one parent is myopic10
![]()
1 in 4
when neither parent is myopic10
Environment
Research shows that a child’s environment and habits may influence the development of myopia.
![]()
Insufficient time spent outdoors.10,11
![]()
Prolonged time spent reading, playing, or working with digital devices, like smartphones or tablets10,12
![]()
Poor lighting levels10,11
In short, more parents with myopia means more children with myopia – and the more that children stay inside and utilize digital devices, the more likely we are to see new myopes.
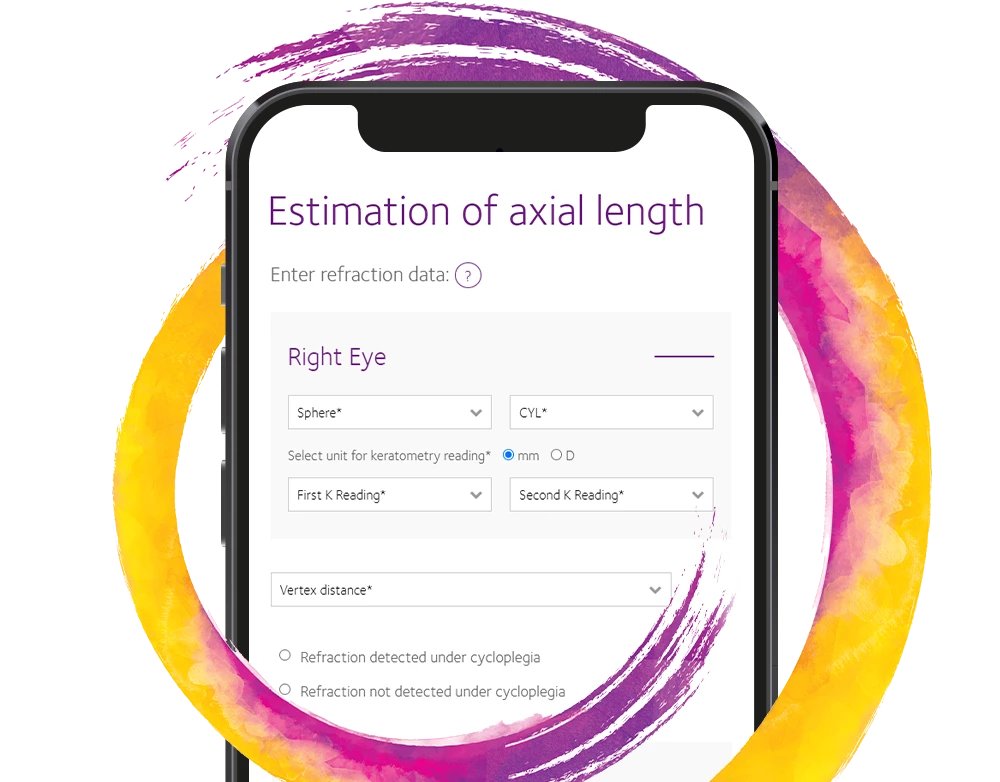
Axial Length Estimator Tool
CooperVision’s Axial Length Estimator can be used to help eye care professionals better understand the significance of ocular axial lengths.
An absence of urgency to address myopia can lead to future risks
Today, only 56% of ECPs agree that myopia, left untreated, increases the risk of irreversible vision loss.‡ But myopic progression has been linked to more severe sight-threatening complications later in life, including13-16:
- Retinal Detachment
- Glaucoma
- Myopic Maculopathy
- Cataracts

CooperVision® is a world leader in myopia control* and management for age-appropriate children
*USA Indications for Use: MiSight® 1 day (omafilcon A) soft (hydrophilic) contact lenses for daily wear are indicated for the correction of myopic ametropia and for slowing the progression of myopia in children with non-diseased eyes, who at the initiation of treatment are 8-12 years of age and have a refraction of -0.75 to -4.00 diopters (spherical equivalent) with ≤ 0.75 diopters of astigmatism. The lens is to be discarded after each removal.
Canadian Indications for Use: MiSight (omafilcon A) Soft Contact Lenses for Myopia Control may reduce the rate of myopia progression in children (6-18) and correct ametropia. Reduction of myopia progression was observed in children with wearing time of 12 hours (8-16 hours) per day, 6.4 days (5-7) per week in a clinical study. Permanent myopia control after lens treatment is discontinued is not supported by clinical studies. MiSight (omafilcon A) Soft Contact Lenses for Myopia Control are indicated for single use daily disposable wear. When prescribed for daily disposable wear, the lens is to be discarded after each removal.
† CooperVision data on file 2019. Myopia Awareness, The Harris Poll online survey 6/27/19 – 7/18/19 of n=313 ECPs (who see at least 1/month myopic child, age 8-15) in U.S. Slightly or significantly increased.
‡ Data on file. CooperVision, Inc. Victor, NY. The Harris Poll online survey of n=1,005 patients (with child age 8-15) and ECPS (who see at least 1 child age 8-15 with myopia each month) in U.S.
§ CooperVision data on file 2019. Myopia Awareness, The Harris Poll online survey 6/27/19 – 7/18/19 of n=313 ECPs (who see at least 1/month myopic child, age 8-15) in U.S. ODs (89%) and MDs (68%) strongly/somewhat agree.]
References:
1. Holden BA, et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology. 2016: 123(5): 1036-1042.
2. Lamoureux EL et al. Mvopia and Ouality of Life: The Singapore Malay Eye Study (SiMES). Invest. Ophthalmol. Vis. Sci. 2008; 49(13): 4469.
3. Chua SYL et al. The Economic and Societal Impact of Myopia and High Myopia. Springer. 2020; 53-63.
4. Tideman JW et al. Association of axial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA Ophthalmol. 2016; 134(12): 1355-1363.
5. Yang, M., Luensmann, D., Fonn, D. et al. Myopia prevalence in Canadian school children: a pilot study. Eye 32, 1042–1047 (2018). https://doi.org/10.1038/s41433-018-0015-5.
6. World Council of Optometry. Resolution: The standard of care for Myopia Management by Optometrists. https://worldcouncilofoptometry.info/resolution-the-standard-of-care-for-myopia-management-by-optometrists/. Accessed January 2024. Canadian Association of Optometrist, Position Statement on Myopia Management. https://opto.ca/document/cao-position-statement-myopia-management. Accessed January 2024.
7. CVI data on file, 2021. Third party provider data breakdown report with 1612 patients between the ages of 8-12 with spectacle x visits and a minimum sphere from both eyes used to defne myopia in US.
8. Statistics Canada. Table 17-10-0005-01 Population estimates on July 1st, by age and sex, https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501.
9. Shah, T., Milosavljevic, S. & Bath, B. Geographic availability to optometry services across Canada: mapping distribution, need and self -reported use. BMC Health Serv Res 20, 639 (2020). https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-020-05499-6.
10. Morgan P. C52102: Is myopia control the next contact lens revolution? 2016. Available from https://www.opticianonline.net/cpd-archive/127.
11. Rose KA, Morgan IG, Ip J, et al. Outdoor Activity Reduces the Prevalence of Myopia in Children. Ophthalmology 2008;115(8):1279-1285.
12. Wolffsohn JS, Calossi A, Cho P, et al. Global Trends in Myopia Management Attitudes and Strategies in ClinicalPractice. Cont Lens Anterior Eye. 2016;39(2):106-16.
13. Xu L, Wang Y, Wang S, Jonas JB. High myopia and glaucoma susceptibility, the Beijing Eye Study. Ophthalmology. 2007;114(2):216-20.
14. Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2013;31(6):622-60.
15. Younan C, et al. Myopia and incident cataract and cataract surgery: the blue mountains eye study. Invest Ophthalmol Vis Sci. 2002;43(12):3625-3632.
16. Chen SJ, et al. Prevalence and associated risk factors of myopic maculopathy in elderly Chinese: the Shihpai eye study. Invest Ophthalmol Vis Sci. 2012;53(8):4868-73.